
The 2026 Crohn’s and Colitis Congress convened clinicians, researchers, and industry partners with the aim to accelerate the translation of new evidence into clinical practice for inflammatory bowel disease (IBD) in Las Vegas, NV from January 22-24th, 2026. Crohn’s and Colitis Congress (CCCongress) offers opportunities for connection and collaboration — which we know are essential for success in driving research and impact for people with IBD. Over the course of three days, the Crohn’s Disease Program team successfully connected with grantees and other leaders in IBD. Check out some team highlights below spanning technology, basic science, clinical practice, and health equity.
Keynote: Developing a Therapeutic for Stricturing Crohn’s Disease

The keynote session delivered by Florian Rieder, MD focused on how strictures (areas of bowel narrowing that often lead to surgery) form in Crohn’s disease, and why they have been so difficult to treat. In his talk, he challenged the long-standing view that fibrosis is a static, irreversible process and stressed the importance of understanding the underlying mechanisms of fibrostenosis to enable the identification and advancement of much-needed, targeted therapeutics for these patients.
Dr. Rieder described how fibroblasts — structural cells that help form tissue — actively respond to inflammatory signals and drive tissue remodeling in the bowel wall. His recent work has shown that specific inflammatory pathways directly activate fibroblasts and promote fibrosis, and that fibroblasts unique to strictures can be targeted to reduce fibrosis. Additional work has shown that mesenteric “creeping fat,” long observed to form specifically at the site of stricture in Crohn’s disease, may contribute to hyperplasia of the smooth muscle, which accounts for most luminal narrowing in stricture formation. Together, these findings highlight that strictures arise from ongoing biological signaling, not just scar tissue left behind after inflammation resolves.
Dr. Rieder emphasized that, despite the progress that is being made in further understanding the disease biology of stricturing Crohn’s disease, to date no anti-fibrotic therapies have been approved for Crohn’s disease. One key barrier has been the lack of validated tools to measure strictures and assess treatment response in clinical trials. This gap led Dr. Rieder and his collaborators at the Mayo Clinic and Alimentiv Inc. to form the Stenosis Therapy and Anti-Fibrotic Research Consortium (STAR), supported in part by Helmsley, which has driven the development of patient-reported outcome instruments and imaging-based indices specifically designed for stricturing Crohn’s disease. These advances have made clinical testing possible and have drawn interest and support from the Pharma and Biotech industries. Through collaboration with STAR, Agomab (Antwerp, Belgium) has recently announced promising results from the first-ever Phase 2a proof-of-concept trial, evaluating a novel anti-fibrotic treatment for patients with stricturing Crohn’s disease. The keynote talk by Dr. Rieder illustrated how coordinated progress across basic biology, measurement standards, and clinical trials is beginning to open the door to therapies aimed at preventing or reversing intestinal strictures.
Therapeutic Chess: Building Consensus in IBD Prescribing
As more therapeutic options become available to people with IBD, medical consensus and shared decision-making will support clearer communication with patients, reduce delays, and promote more consistent, personalized care.
The “Therapeutic Chess” session centered on a single patient case study to explore how clinicians approach treatment selection in complex IBD scenarios. Audience members were asked to vote on which therapy they would prescribe, after which panelists defended different choices and talked through the clinical reasoning behind each option. The exercise made clear that differences in prescribing were not rooted in disagreement about treatment goals, but in how individual providers weighed patient-specific considerations including disease activity, comorbidities, and prior therapy history.
As the discussion unfolded, panelists highlighted how different patient characteristics, such as age, cardiovascular risk, pregnancy considerations, extraintestinal manifestations, or safety history, could justifiably shift treatment choice from one agent to another. The session also surfaced the practical realities that shape prescribing, including insurance approval processes, documentation requirements, and access to patient assistance programs. By making both clinical nuance and healthcare barriers explicit, the session reinforced the complexities of treating IBD and why transparent, team-based approaches are essential for ensuring quality care.
Advancing Basic Science in IBD
Understanding the biological mechanisms of disease onset and progression provides the foundation for new therapeutic, diagnostic, and preventative strategies towards treating and ultimately curing Crohn’s disease. Basic science sessions at CCCongress focused on the complex communication between immune, epithelial, stromal, and neuronal cells, as well as the role of physical and environmental cues such as mechanical forces and the microbiome in mediating disease onset and progression.
Collectively, these talks underscored the need to study CD as more than an immune disorder. Advanced experimental models and technologies that characterize a single cell’s behavior in exquisite detail within patient-derived tissues have opened the aperture that allows investigators to view the complexities of disease biology – a fundamental step towards finding a cure.
Intestinal Ultrasound: A Faster Path to Clinical Decisions
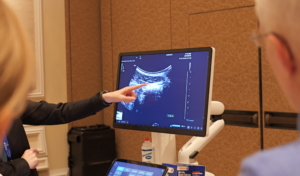
iUSCAN sessions highlighted intestinal ultrasound (IUS) as a tool that can significantly shorten time to meaningful clinical decisions in IBD care. IUS is a non-invasive, patient-friendly, point-of-care imaging tool that is effective at confirming active disease, allowing clinicians to make quick and informed decisions around therapeutic intervention at the point of care.
Speakers emphasized that IUS is well suited for most people with IBD, including pediatric and pregnant patients, enabling repeat, real-time assessment of bowel wall thickness and inflammatory activity. Faster results reporting has been linked to higher patient satisfaction, as care plans that can be adjusted more quickly in response to objective findings.
Importantly, IUS is increasingly embedded in IBD research and clinical guidance, including the STARDUST sub-study and its inclusion in ECCO and PIANO recommendations. At Helmsley, we’ve invested in efforts to expand the evidence base for IUS and support its integration into clinical research and practice, reflecting the growing recognition of its potential to improve patient care. While challenges remain, particularly around training, standardization, and implementation costs, the sessions made clear that wider adoption of IUS represents a practical opportunity to speed diagnosis, monitoring, and treatment decisions in IBD.
Shaping the Future of IBD Care
Advancing progress in IBD care depends on alignment across disciplines, from fundamental biology to clinical decision-making and equitable access. CCCongress offered a clear view of where the field is headed and what will be required to deliver real-world solutions that give people with IBD better and more accessible treatment options, underscoring that lasting impact will depend on sustained investment in the research infrastructure needed to move new ideas from discovery into practice.
CCCongress is organized by the Crohn’s and Colitis Foundation and the American Gastroenterological Association.


